I never thought that 77.1% of women’s success or failure of the test tube, but depends on this small step before transplantation!
What do you need to pay attention to before transplantation, it is estimated that a thousand sisters have 10,000 kinds of views, some have a scientific basis, and some may be just rumours, the circle sister once gave some precautions before and after the transplantation, but it is not comprehensive.
This article to say this precaution, it is estimated that nine out of ten sisters have not heard of, perhaps even the doctor has not been concerned about, but this really affects the success rate of pregnancy, so it must be said clearly.
Let me ask you a question: Has anyone ever checked their thyroid function before transplantation? I’m guessing very few of you can give an affirmative answer, it’s a matter of pregnancy success or failure.
You may say, I have checked the thyroid gland is not a problem, but IVF itself can cause thyroid abnormalities, let’s take a look at what the literature says.
01 IVF affects thyroid function
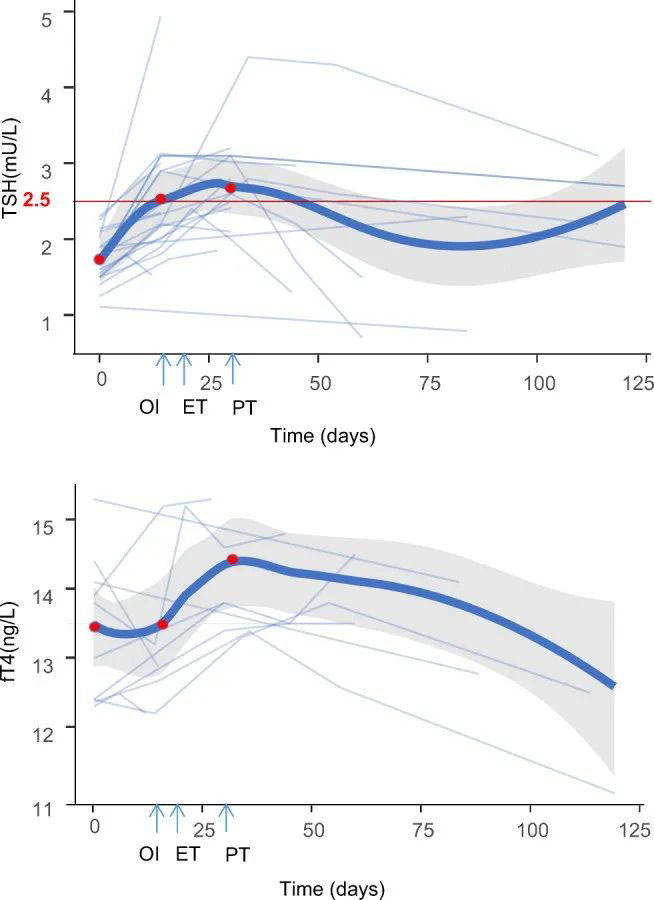
This is a meta-analysis article published in the Journal of Assisted Reproduction and Genetics, the total sample size was 1,665 individuals, and the average TSH value at the end of the IVF was 2.53, which doesn’t seem high, but note that this is the average.
What’s worse is that this state persisted, consistently above the threshold, for a full month, which corresponds to one month post-transplantation, severely impacting pregnancy success.
Elevated TSH, commonly known as hypothyroidism, makes it difficult for a woman to get pregnant.
If a woman becomes pregnant, her body is severely deficient in thyroxine, and the foetus relies on the mother’s supply of thyroxine, which can lead to miscarriage or serious malformation of the foetus.
Even if pregnancy is successful, as thyroid function directly affects mental ability, hypothyroidism is likely to cause foetal retardation, mental retardation, preterm delivery, intrauterine foetal death, gestational toxicity, etc., and hereditary possibilities.
In vitro fertilisation can overstress the hypothalamic-pituitary-thyroid axis, which can lead to compensatory increases in thyroid hormone (TSH).
In this study, TSH levels rose in 63.3-77.1% of women who underwent boosting.
In the case of fresh embryo transfer, then after ovulation and egg retrieval, the interval of three to five days is the day of transfer, and in between, it is assumed that few people will think to check thyroid function, but by this time, thyroid function is already in a state of hypothyroidism, which affects the outcome of the embryo transfer.
What is even more frightening is that this hypothyroidism lasts for a month, which can make it difficult for the embryo to implant, or biochemistry or miscarriage after implantation, and if pregnancy occurs it may result in a thyroid deficiency in the foetus, causing other adverse consequences.
Therefore, for patients with fresh transfer after ovulation induction, thyroid function tests need to be performed at the end of ovulation induction; if abnormal, medication is adhered to after transfer.
Or cancel the fresh embryo transfer and wait for frozen embryo transfer to give thyroid function a recovery time.
02 Our authoritative literature gives another conclusion
Compared with meta-analysis, this retrospective case study published in China’s Chinese Journal of Reproduction and Contraception is a direct clinical summary of the same findings, giving a different conclusion.
Their number of cases was 124, mainly for patients with subclinical hypothyroidism who were already on medication, divided into two groups, with positive auto-thyroid antibodies as one group and negative as another.
I’m not going to list the exact data and give you the conclusions.
They measured tsh values at three time periods, before the start of ovulation promotion as baseline TSH values, on hcg day, which is before egg retrieval, and 14 days after transplantation.
They found that TSH levels were significantly higher in the clinically pregnant group than in the non-pregnant group, and that the increase in TSH levels after ovulation was more pronounced in the thyroid autoantibody-positive group compared to the thyroid autoantibody-negative group.
This study also suggests, as did the previous study, that induction has a significant effect on thyroid function in all patients, regardless of prior hypothyroidism.
Unlike the previous study, this study tells us that the effect is more pronounced at 14 days after embryo transfer and that TSH levels above the threshold (4.2 mU/L) at 14 days after embryo transfer are often indicative of a successful assisted pregnancy.
In cases where TSH is mildly elevated during ovulation induction, the oestradiol level will have partially decreased by the time a pregnancy is not achieved at 14 days after embryo transfer, and the TSH level may have decreased to normal.
The experts in this study therefore recommend that thyroid function should be reassessed before ovulation induction and again 14 days after embryo transfer, if possible, to minimise overtreatment and unnecessary medical costs.
In addition, although pregnancy outcomes did not differ between groups with different TSH control levels at baseline, those with TSH <2.5 mU/L had a reduced risk of a significant increase in TSH levels after ovulation.
In order to minimise the possible adverse effects of subclinical hypothyroidism on pregnancy, it is therefore recommended that TSH levels be controlled to 2.5 mU/L or less prior to augmentation.
Finally, the study also showed that TSH levels changed more dramatically in thyroid antibody-positive patients during ovulation, and that in positive patients, serum TSH levels were significantly higher than in negative patients at 14 days after embryo transfer.
These results confirm that thyroid autoantibody-positive patients have reduced thyroid reserve function, and that the effect of ovulation on thyroid function is more pronounced in positive patients.
03 What these two studies tell us
These two studies may seem to have different conclusions at first glance, but they are in fact similar, not contradictory at all, and complementary to each other.
The first study looked at all patients, both those with and without thyroid problems, while the second study looked at patients with subclinical hypothyroidism who were already on medication.
What these two studies have in common tells us that boosting causes hypothyroidism, which lasts for about a month, with the most pronounced elevation at 14 days after transplant.
If you are pregnant, the TSH elevation is even more pronounced, but this elevation is actually detrimental to the pregnancy and requires intervention, and the big difference between these two studies is when exactly to start intervention.
The first study considers checking thyroid function before transplantation and intervening promptly if there is an elevation;
Whereas the second one argues that it’s significantly elevated at 14 days, and it’s okay to go ahead and intervene at that point, arguing that the safest thing to do is to get the TSH down to a complete level, preferably below 2.5, before ovulation.
So the main difference in their claims is in the timing of the intervention, whether to intervene before ovulation or to detect the elevation at the beginning of the transplant and then intervene.
I think it may have something to do with the population they are dealing with, if you have no thyroid problems before ovulation, you can wait until the time of transplantation to be concerned.
If you have a thyroid problem yourself, then you need to play ahead and try to avoid boosting if your TSH doesn’t drop below 2.5 so as not to affect the pregnancy outcome.
In short, this article is trying to tell you that IVF boosting affects thyroid function and can easily cause hypothyroidism!
If you have hypothyroidism yourself, you must take care of your thyroid before the transplant.
Even if you don’t have a thyroid problem yourself, the boost can directly cause a hypothyroid condition!
If you are going to have a fresh embryo transfer, make sure you don’t forget to check your thyroid function and take the medication you need to make sure that your thyroid is not affecting the outcome of your pregnancy.
If you have hypothyroidism yourself, ovulation may exacerbate it, so be sure to adjust your medication appropriately based on the test results!
The thyroid gland is the organ most affected by hormone fluctuations, so don’t let it affect the big picture, as one careless move can easily lead to a total loss!
Please take care of the thyroid gland before and after the transplant!